

Summary of Colorado Option Standardized Plan Stakeholder Meetings: Updated on 10/7
Introduction
In accordance with House Bill 21-1232, signed into law by Governor Jared Polis, the Colorado Division of Insurance (DOI) must develop the standardized health benefit plan (i.e., Colorado Option) – slated to go live on January 1, 2023 – with input from a diverse cross-section of organizations and communities. Over the next several months, DOI will convene six stakeholder engagement meetings to discuss the framework for the standardized plan, culminating in a final rule. The final rule must be adopted by January 1, 2022.
Notably, DOI is gathering stakeholder input on a relatively accelerated timeline in order to submit a 1332 state innovation waiver application to the Centers for Medicare and Medicaid Services (CMS) by November 30, 2021. Through the federal waiver, DOI would receive pass-through funding from savings generated by implementation of the standardized health benefit plan. The savings will be directed to Colorado’s reinsurance program, administered by the Colorado Health Insurance Affordability Enterprise, and used to increase the value, affordability, quality, and equity of health care coverage for all Coloradans.
Scope of Stakeholder Engagement Process
The stakeholder engagement process is primarily focused on the design of the standardized health benefit plan – specifically:
Actuarial Value (how much does plan pay vs. how much person pays);
Cost-sharing (coinsurance vs. copay; how much?); and
Reducing racial health disparities through plan design.
DOI will pursue a separate stakeholder process regarding provider network requirements. Additional details about other components of the Colorado Option – mandatory cost-sharing reductions and 1332 state innovation waiver – are available in our summary of House Bill 21-1232.
Timeline

Standardized Health Benefit Plan
House Bill 21-1232 requires insurance carriers to offer the standardized health benefit plan through the Exchange (i.e., Connect for Health Colorado; individual and small group markets) and through the Public Benefit Corporation (individual market), beginning in plan year 2023. Carriers must offer the standardized plan at a premium rate that is at least five percent less than the premium rate offered in 2021 in each of the first three years of offering the standardized plan, resulting in a 15 percent premium reduction in plan year 2025 compared to plan year 2021. For plan year beginning 2026 and subsequent years, the carrier must limit any annual premium rate increase to no more than medical inflation relative to the prior year.
Additionally, the law sets broad parameters for the design of the standardized health benefit plan.
Metal Tiers: Offers coverage at the gold, silver, and bronze levels.
Benefits: Covers essential health benefits (EHBs) required by the Affordable Care Act (ACA) and Colorado.
Racial Health Equity: Is designed to improve racial health equity and decrease racial health disparities through strategies, including –
Perinatal health care coverage; and
First-dollar, pre-deductible coverage for certain high-value services, such as primary care and behavioral health care.
Provider Network Adequacy: Has a network that is culturally responsive, representative of the community it services, and not narrower than the most restrictive network that the carrier is offering in the same area and same metal tier.
Other design considerations identified by DOI are market competition and value-based insurance design. The stakeholder engagement process will determine, at a more granular level, the cost-sharing and benefit design.
Key Takeaways from Stakeholder Meetings (schedule and materials available here)
July 29th: Meeting #1 – Overview of the Legislation and Stakeholder Engagement Process
DOI staff welcome feedback on the design of the standardized health benefit plan through various channels – public comments at stakeholder engagement meetings, email (dora_ins_co_option@state.co.us), and Google forms for future meetings. The rulemaking process will also entail a public comment period. Michael Conway, Colorado Insurance Commissioner, emphasized his openness to feedback and intent to have “productive conversations.”
Kyle Brown, Deputy Commissioner for Affordability Programs, is DOI’s point person for stakeholder engagement (Kyle.m.Brown@state.co.us). Other DOI staff contacts are:
Cara Cheevers, Behavioral Health Program Director (Cara.Cheevers@state.co.us);
Debra Judy, Deputy Commissioner for Policy Affairs (Debra.Judy@state.co.us); and
Leilani Russell, Health Initiatives and Implementation Project Manager (Leilani.Russell@state.co.us)
Colorado’s standardized health benefit plan may draw from existing standardized plans. Brown noted the availability of standardized plans in seven states (California, Connecticut, Massachusetts, New York, Oregon, Vermont, and Washington) and the District of Columbia as well as common elements featured in those plans – including: deductible, out-of-pocket maximum, and copay or coinsurance for services (see slides 18 and 19). Of note, CMS intends to propose standardized plan designs in the forthcoming 2023 notice of benefit and payment parameters, according to the third installment of the ACA payment parameter updates for 2022. How this plan will affect Colorado’s standardized health benefit plan is unclear at this point.
The stakeholder engagement process will examine the trade-offs of various plan designs – i.e., between coverage and cost-sharing within the bounds of the metal tiers. Specific questions noted by DOI include:
If certain services are pre-deductible, what cost sharing must increase to maintain actuarial value?
How does actuarial value impact premium?
Where should Colorado target the actuarial value for the standardized plan
DOI has contracted (or will contract) with a firm to conduct actuarial analysis. Another consideration that will be analyzed is the interaction between standardized health benefit plans and premium tax credits.
DOI’s strategies for reducing health disparities include first-dollar, pre-deductible coverage or incentives for certain high-value services. The law does not define “high-value services,” and therefore DOI seeks stakeholders input on identifying these high-value services. The third meeting will focus on this issue.
The same standardized health benefit plan will be offered in the individual and small group market, but carriers may be given some flexibility that allows for variation within plans, according to Brown. The plan is unlikely to include benefits beyond EHBs.
DOI aims to finalize the rule establishing the standardized health benefit plan by November, for purposes of informing the 1332 state innovation waiver application, and may be released as soon as September, according to Brown. He acknowledged that the release may be delayed depending on stakeholder engagement.
August 13th: Meeting #2 – Required Benefits and Introduction to Cost-Sharing and Benefit Design
1. The standardized plan will cover Essential Health Benefits (EHBs) as defined in Colorado’s benchmark plan, which may include additional benefits if approved by the Centers for Medicare and Medicaid Services (CMS). DOI recently submitted the following proposed changes to Colorado’s benchmark plan:
Adding acupuncture – covering up to six visits per member per benefit year
Adding gender affirming care;
Adding a mental wellness exam – covering one 45-60 minute visit per year that includes services such as behavioral health screening, education and consultation on health lifestyle change, referrals to ongoing mental health treatment, and discussion of potential options for medication; and
Expanding the required number of drugs covered for certain United States Pharmacopeia (USP) classes, also referred to as “Alternatives to Opioids” or ALTOs.
The final determination is expected this summer. If approved, the revised benchmark plan will become effective for 2023 (when the standardized plan is also slated to take effect).
2. To design a standardized plan that meets the parameters of covering EHBs and offering coverage at the gold, silver, and bronze levels, DOI is examining tradeoffs between premiums and cost-sharing – (1) higher actuarial value plans with higher premiums and lower cost-sharing; or (2) lower actuarial value plans with lower premiums and higher cost-sharing. Advancing racial health equity is a top consideration for DOI – specifically, more coverage (i.e., lower cost-sharing) for high-value services.
A consumer advocate noted that “people often get subsidies for premium,” emphasizing that the standardized plan should prioritize lower cost-sharing over lower premiums. A broker in favor of a standardized plan with lower premiums pointed out that the lack of transparency around actual health care costs makes it difficult to figure out the actual cost-sharing amount.
DOI is looking to stakeholders for input in identifying high-value services. The next meeting will focus on how incentivizing high-value care, presumably through first-dollar coverage or lower cost sharing, can reduce health disparities and improve health equity.
3. One challenge to identifying high-value services at the plan level is selecting a specific set of services considered to be high value that addresses the needs of a diverse population. Whether DOI will build flexibility into the standardized benefit plan that allows health care providers to decide which services are high value for their patients remains to be seen. A family physician from the Colorado Medical Society noted that the context for the patient must be considered (e.g., a specific drug may be considered high value for one patient but not another patient). Another physician emphasized the need to consider accessibility, such as distance and travel time, when determining high-value services.
4. DOI will host additional meetings with specific stakeholder groups for more focused discussions on the design of the standardized plan. DOI will meet with:
Consumer groups and community members;
Hospitals and other health care facilities;
Providers;
Health plans (Brown also noted that DOI will meet with brokers; and
Rural entities and community members.
September 9th: Meeting #3 – Incentivizing high-value care: How can it reduce health disparities and improve health equity?
1.To meet the statutory requirement that the standardized plan be designed to reduce health disparities and improve racial health equity, DOI sought input on (1) which health disparities should be prioritized and addressed; and (2) evidence-based approaches that can be incorporated into the plan design. The Colorado Department of Public Health and Environment (CDPHE) and consumer advocates (Colorado Consumer Health Initiative and Colorado Center on Law and Policy) presented considerations for plan design that generally aligned with one another.
2. Overall, CDPHE and consumer advocates identified the same or similar health disparities.
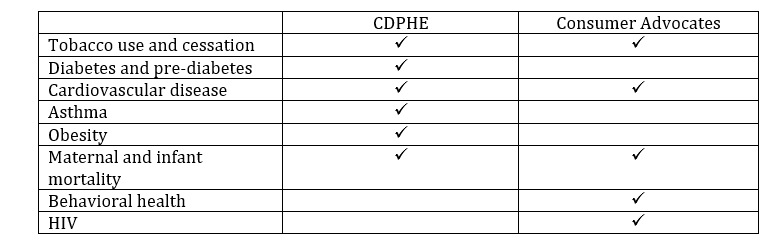
3. Stakeholders discussed a variety of plan design considerations to address the identified key health disparities – e.g., which services to cover, when to waive cost-sharing.
4.Consumer advocates emphasized their preference for copay rather than coinsurance, noting “copay structures create transparency.” Additionally, they called for relatively low deductibles. Their presentation states, “Most Coloradans identify any deductible above $1,000-$2,000 as unaffordable/causing financial hardship.”
5.Consumer advocates cautioned against using the term “low-value services,” explaining that “certain services that are deemed low-value services may be considered higher value for communities of color.” They cite an article published in the Health Affairs Blog (May 21, 2021) that calls on the broader health care and health policy community to recognize the role of systemic racism in health outcomes and for a “re-examination of what low-value and high-value care means to the well-being of communities of color.”
September 24th: Meeting #4 – Plan Design and Cost Sharing Part 1
1.To inform the design of the standardized plan, DOI is looking at what plans people are currently buying. Notably, the most recently available information is from 2019, which does not reflect the impact of enhancements to premium tax credits (made available by the American Rescue Plan Act of 2021, P.L. 117-2). Among plans with highest enrollment, some common themes emerged:
There is a mixture of copays typically for highly utilized services and coinsurance typically for higher cost, lower utilized services.
Primary care visits, generics, and urgent care offered prior to deductible.
On actuarial value (AV), gold plans tended to span the de minimis range, while silver plans were more concentrated in the lower half of the required range and bronze plans were more concentrated at the high end of the required range.

2.Stakeholder feedback is coalescing around some common themes that generally align with consumer behavior.
Support copay cost-sharing structure to facilitate price transparency and predictability.
Balance lower premiums with maximizing subsidy amounts for eligible individuals.
Incentivize primary care visits, generic drugs, and behavioral health visits through no to low cost-sharing limits.
3. Julie Peper from Wakely presented draft plan designs at the gold, silver, and bronze metal levels. The sample plan designs were intended to “facilitate discussion around the structure and priorities for plan design as well as the potential trade-off between cost sharing and AV/premiums.” Based on the examples presented, the main decision points appear to be:
Whether to pursue a plan that prioritizes the use of copays over coinsurance (or vice versa). Peper explained, “Plan designs with more fixed elements, such as copays, will likely require more substantial updates year over year to maintain compliance with AV requirements versus a plan design that is largely coinsurance-based, where the value of the member cost sharing increases proportionately to the underlying claim cost.” DOI is unlikely to view the need to annually update the standardized plan as a downside, since Commissioner Insurance Commissioner Michael Conway has indicated that there will be an annual process to update the standardized plan.
Which benefits will be available prior before the deductible. These benefits will likely reflect benefits that DOI views will improve racial health equity.
4. Deputy Insurance Commissioner Kyle Brown signaled that DOI will soon release the proposed regulation establishing the standardized plan (possibly in early October). There will be a public comment period. DOI aims to finalize the regulation by November ahead in order to submit a 1332 state innovation waiver application to CMS by November 30, 2021.
With support from Arnold Ventures